Processing Disorders
תיאור הקורס
קיים בלבול רב בקרב אודיולוגים ופתולוגים בשפה הדיבור כאשר מוצגת אבחנה של "הפרעת עיבוד". קורס זה מציג מודל רצף להבדיל הפרעות עיבוד להיבטים אקוסטיים, פונמיים או לשוניים, כך שהערכה וטיפול יכולים להיות ממוקדים ויעילים יותר. מתוארים תפקידיהם של אודיולוגים ו-SLPs ביחס להפרעות עיבוד, ומוצגות אסטרטגיות פיצוי להיבטים שונים של עיבוד.
מהשולחן של אן קאמר
אני כל כך נרגש מהמאמר הזה ב-20Q כי שם
ממשיך להיות הרבה בלבול בין שניהם
אודיולוגים ופתולוגים בדיבור
לגבי האבחנה של "הפרעת עיבוד". אָנוּ
השתמש במונחים כגון "הפרעת עיבוד שמיעתי",
"הפרעת עיבוד שמיעתי מרכזי", "שפה
הפרעת עיבוד" ו"הפרעת עיבוד פונמית", אבל לא תמיד ברור לנו
כיצד ההפרעות והמונחים הללו מובדלים. למרבה המזל, ד"ר גייל ג'יי ריצ'רד, Ph.D.,
CCC-SLP יענה על השאלות שלנו לגבי הפרעות עיבוד עם מאמר 20Q זה.
הנה מידע קטן על ד"ר ריצ'רד. היא פרופסור אמריטוס באוניברסיטת מזרח אילינוי בצ'רלסטון, אילינוי, שם הייתה בפקולטה במשך 37 שנים והתמחתה בהפרעות שפה התפתחותיות בילדות, כגון הפרעות בספקטרום האוטיסטי, עיבוד שמיעה/שפה, תפקודים ניהוליים ואילמות סלקטיבית. היא גם הקימה את המרכז לאוטיזם באוניברסיטה ותוכנית לסטודנטים עם הפרעת הספקטרום האוטיסטי - Students with Autism Transitional Education Program (STEP). יש לה פרסומים רבים והיא מגישה כנסים תדיר, וחולקת את נקודת המבט הקלינית המעשית שלה. פרסים מקצועיים כוללים כבוד של האגודה האמריקאית לדיבור-שפה-שמיעה, זוכה פרס ההישג הקליני של אילינוי ופרסי הוראה מרובים. היא גם מילאה תפקידי מנהיגות רבים בארגונים מקצועיים, כולל נשיאת האגודה האמריקאית לדיבור-שפות-שמיעה ב-2017.
במאמר זה, ד"ר ריצ'רד ישתמש ברצף כדי להסביר הפרעות עיבוד הכוללות היבטים אקוסטיים, פונמיים ו/או לשוניים. היא דנה באחריות של אודיולוג ופתולוג שפת דיבור ביחס להפרעות עיבוד. והכי חשוב, היא נותנת דוגמאות של מיומנויות ספציפיות ואסטרטגיות פיצוי שניתן להשתמש בהן עבור הסוגים השונים של הפרעות עיבוד.
קורס זה בהחלט יעזור לך להבדיל בין הפרעות עיבוד על סמך היבטים אקוסטיים, פונמיים או לשוניים. כתוצאה מכך, ההערכה והטיפול שלך יהפכו ממוקדים ויעילים יותר.
עכשיו... המשך לקרוא, למד ותהנה!
תוצאות למידה
לאחר קורס זה, הקוראים יוכלו:
להגדיר ולהבדיל הפרעות שמיעה ועיבוד שפה
נצל רצף כדי לתאר היבטים שונים של עיבוד לאקוסטי, פונמי ולשוני זיהוי האחריות של אודיולוג ופתולוג שפת דיבור ביחס להפרעות עיבוד ציין דוגמאות של מיומנויות ספציפיות ואסטרטגיות מפצות בהיבטים האקוסטיים, הפונמיים והלשוניים של מעבד
1. מהי "הפרעת עיבוד?"
"הפרעת עיבוד" היא למעשה מונח כללי המשמש אנשי מקצוע רבים לתיאור מגוון בעיות למידה. פסיכולוגים, מורים, אודיולוגים ופתולוגים של שפת דיבור כולם מציגים את המונח כאשר אדם מתקשה בצורה מדויקת
הבנה ותגובה למידע חושי. למרבה הצער, ישנן מספר מיומנויות שונות המוכללות במונח "הפרעת עיבוד" מה שמוביל לבלבול רב.
2. האם ישנם סוגים שונים של הפרעות עיבוד?
בהחלט! אנו מעבדים מידע מכל מערכות החישה שלנו. אנחנו יכולים לעצום את העיניים ולטעום, להריח או להרגיש משהו כדי לנסות ולהבין מה זה. בספרות אפזיה, אנו מדברים על אגנוזיה - כאשר אתה מקבל גירוי אבל לא יכול להבין או להבין אותו. קל יותר להבין אותו בחושי הראייה (הראייה), המישוש (המגע), הריח (הריח) והטעם (הטעם), כי הם נשארים שם בזמן שאתה עובד על הצמדת משמעות לגירוי. מידע שמיעתי קשה יותר לעיבוד מכיוון שהוא כל כך חולף - הוא נעלם מהר מאוד. לאחר מכן נוסיף את ההיבט של מידע שמיעתי בקוד שפה. מלבד רעשי סביבה, גירויים שמיעתיים דורשים יותר אנרגיה קוגניטיבית כדי להבין. רוב האתגרים המשפיעים לרעה על הלמידה והתפקוד בעולם היומיומי הם בתחום העיבוד השמיעתי.
3. מהו עיבוד שמיעתי?
כאשר "עיבוד שמיעתי" הוצג לראשונה (Mylebust, 1954) הוא שימש לתיאור ילדים עם שמיעה תקינה אך נאבקו להבין מידע שמיעתי שהוצג בפניהם. הם יכלו לשמוע את המילים אבל התקשו לייחס משמעות כדי להבין את המסר בתוך השפה. המונח היה רחב מאוד בהגדרתו. זה התייחס להפרעה בהבנת השפה שיכולה להתבסס על שפה, למידה אקדמית או מיומנויות הקשבה. במשך עשרות שנים המונח "עיבוד שמיעתי" הוגדר כבעיות בהפשטת משמעות מגירוי שמיעתי (Massaro, 1975), שהקיף יכולות קוגניטיביות ושפה רבות.
עם התפתחות תחום האודיולוגיה, אנשי מקצוע רצו להבדיל טוב יותר בין מרכיבי השמיעה והשפה. הצעד הראשון היה להדגיש שהאדם חייב להיות בעל חדות שמיעה תקינה במערכת השמיעה ההיקפית. במילים אחרות, האדם יכול לקבל במדויק גירוי שמיעתי אך מתקשה להבין או לפרש את האות. "עיבוד שמיעתי מרכזי" הוצג (Keith, 1977) כדי לציין שהליקויים התבססו על מיומנויות שמיעתיות המתווכות במערכת העצבים השמיעתיים המרכזית (CANS). הקושי להבחין בתכונות שונות של האות האקוסטי הפריע לאחר מכן להבנת המסר.
4. למה אתה מתכוון בתכונות אקוסטיות של האות?
כאשר אנו מנתחים גירוי אקוסטי, ישנם היבטים רבים התורמים לשלמות הצליל. גובה הצליל, העוצמה, מהירות ההצגה והפונמות השונות מתרחשים יחד במהירות רבה. אדם צריך להיות מסוגל להבחין בין מקטעי הצליל השונים כדי לייחס במדויק משמעות. לדוגמה, אני צריך להיות מסוגל לשמוע את ההבדל בין "p" לעומת "b" כדי לדעת אם המילה ששמעתי היא "פט" או "עטלף". הפרשנות שלי להודעה תהיה מבולבלת אם לא אוכל להבדיל בין הצלילים הללו. התמונה במוח שלי תיווצר על ידי האופן שבו אני שומע ומפרש רצף קול. לרצף הצלילים תהיה משמעות המבוססת על קוד השפה.
5. האם תוכל לתת לי כמה דוגמאות לכישורים האקוסטיים שהם חלק מהפרעת עיבוד שמיעתי?
אודיולוג יחפש ביצועים גרועים ביכולת לוקליזציה של צליל, יכולת להבחין בפונמות שונות, בעיות בשמיעה כאשר האות נפגע על ידי רעשי רקע או סטטיים, או בעיות בשמיעה כאשר יש יותר מסיגנל אחד בו-זמנית.
6. האם המאפיינים האקוסטיים הם חלק מההגדרה להפרעת עיבוד שמיעתי מרכזי?
כן, אודיולוגים ופתולוגים של שפת דיבור הכירו בהדרגה שיש היבטים אקוסטיים, פונמיים ולשוניים לעיבוד. אודיולוגיה התמקדה בהיבטים האקוסטיים והפונמיים של עיבוד שמיעתי. מבחינה נוירולוגית ההגדרה שלהם התמקדה בהעברת האות האקוסטי מהאוזן הפנימית דרך מערכת העצבים השמיעתית המרכזית לקורטקס העליון. ההגדרה לעיבוד שמיעתי היא "העיבוד התפיסתי של מידע שמיעתי במערכת העצבים המרכזית (CNS) והפעילות הנוירוביולוגית העומדת בבסיס עיבוד זה ומביאה לפוטנציאל שמיעתי אלקטרו-פיזיולוגי (ASHA, 2005a). בעיקרון, עיבוד שמיעתי הוא היעילות והאפקטיביות באופן שבו מערכת העצבים השמיעתית המרכזית מנצלת מידע שמיעתי.
7. האם "עיבוד שמיעתי" ו"עיבוד שמיעתי מרכזי" זה אותו דבר?
כן, יש הסכמה באודיולוגיה שאלו מונחים נרדפים. במשך זמן מה המרכז נכלל בסוגריים, כך שתראה עיבוד שמיעתי (מרכזי) או (C)AP. זה היה כדי להדגיש את ההתמקדות במיומנויות מערכת העצבים השמיעתית המרכזית (CANS) כאשר מתייחסים להפרעה בעיבוד שמיעתי. ההמלצה (ASHA, 2005b) הייתה להוריד את המרכז ולהשתמש רק בעיבוד שמיעתי (AP) והפרעת עיבוד שמיעתית (APD) ללא שימוש במרכז.
8. מי יכול לאבחן הפרעת עיבוד שמיעתי?
אודיולוג הוא איש המקצוע היחיד שיכול לאבחן הפרעה בעיבוד שמיעתי. בעוד שאנשי מקצוע רבים עשויים להציע שלאדם יש הפרעת עיבוד שמיעתי, הם מתארים את סוגי הפעילויות הבעייתיות עבור אדם. מורה, פסיכולוג או רופא עשויים להבחין שאדם מתקשה להבין את הנאמר להם ולציין שיש לו הפרעת עיבוד שמיעתי, אבל זו לא אבחנה. זו חוות דעת מקצועית מה יכולה להיות הבעיה. יש לשקול הפניה להערכה רשמית.
9. מה כוללת ההערכה להערכת הפרעת עיבוד שמיעתי?
מטרת הערכת עיבוד שמיעתי היא להעריך את שלמות מערכת העצבים השמיעתית המרכזית באופן דיסקרטי מבוקר. הבדיקות מדגישות את מערכת השמיעה על ידי פגיעה באות האקוסטי כדי לראות כיצד האדם מגיב. כל אודיולוג מעצב סוללת בדיקות שלדעתו יעריכו בצורה נאותה את יכולת העיבוד השמיעתי של הפרט. ישנם ארבעה סוגים של נהלים שניתן להשתמש בהם בהערכת עיבוד שמיעתי מרכזי:
מונוטי/מונורלי – גירויים אקוסטיים המוצגים לאוזן אחת;
דיכוטי – גירויים אקוסטיים שונים המוצגים בו זמנית לשתי האוזניים, כגון "חם" באוזן שמאל ו"כלב" באוזן ימין בו זמנית;
אינטראקציה בינאורלית – יש להוסיף או להפריד אותות נפרדים לכל אוזן, כגון "m" לאוזן שמאל, "a" לאוזן ימין ו-"t" לשמאל למילה "mat";
אלקטרופיזיולוגיות - אלו בדיקות רפלקס נוירולוגיות שאינן דורשות תגובה מהפרט; אלקטרודות מחוברות להערכת תגובות גזע המוח.
אין סוללת הסכמה באודיולוגיה לגבי המיומנויות שיש לכלול בהערכה. עם זאת, כלל האצבע לאבחון הפרעת עיבוד שמיעתי הוא ליקוי בביצועים של 2 סטיות תקן מתחת לממוצע בשתי בדיקות או יותר של הסוללה שניתנו לאדם.
10. מה תפקידו של פתולוג שפת הדיבור בהפרעות עיבוד שמיעתי APD?
בעוד שאודיולוג אחראי על אבחון הפרעת עיבוד שמיעתי, לרוב מדובר בפתולוג בשפה הדיבור (SLP) שאחראי על תיאום ומתן טיפול לטיפול בליקויים בעיבוד השמיעה. לכן חשוב לדעת אילו מיומנויות שמיעה נפגעו באופן משמעותי שהביאו לאבחון APD. ישנם היבטים רבים להערכת עיבוד שמיעתי הבוחנים את יכולתו של האדם להבחין בתכונות אקוסטיות שונות. ה-SLP צריך לעבוד עם האודיולוג כדי לזהות את ההיבטים הרלוונטיים ביותר שיעשו את ההבדל מבחינה תפקודית.
11. מה ההבדל בין עיבוד שפה לעיבוד שמיעתי?
עיבוד אות אקוסטי שונה מאוד מעיבוד אות לשוני. עיבוד שמיעתי דורש בדרך כלל פרשנות מועטה עד מינימלית של הגירוי השמיעתי. לפעמים מטלת חזרה פשוטה תגיד לך שהאות הועבר בצורה מדויקת דרך גזע המוח לקליפת המוח העליונה. למערכת העצבים המרכזית יש יתירות נוירולוגית מדהימה שממזערת את האפשרות של חוסרים בהעברת האות לאונה הטמפורלית. רוב הפרעות העיבוד השמיעתי מתרחשות ברגע שהאדם מתחיל להבחין ולתפעל את התכונות האקוסטיות בקליפת המוח העליונה ברמה פונמית. האות האקוסטי הוא בדרך כלל לא מקור הבעיה. הקושי הוא כאשר הפרט מנסה לפענח ולפרש את המסר בתוך האות השמיעתי. זה עיבוד שפה. עיבוד שפה הוא היכולת לייחס משמעות לגירוי האקוסטי. זוהי היכולת להבין את המסר הסמנטי והתחבירי המקודד באות. רבים מקשיי הלמידה שחווים ילדים במסגרת אקדמית מבוססים על קושי בעיבוד שפה.
12. מי מאבחן הפרעות בעיבוד שפה?
פתולוג שפת הדיבור אחראי על ביצוע הערכה כדי לראות אם הליקויים הם בהיבטים פונמיים או לשוניים של העיבוד. פתולוג שפת הדיבור יערוך הליכי הערכה כדי להעריך אפליה פונמית ומניפולציה של צלילים וכן הבנת השפה. אין מכשיר הערכה אחד שיספק את המידע הדרוש, ולכן ה-SLP חייב להסתמך גם על סוללת בדיקות, כמו מה שעושים האודיולוגים בהערכה. ישנן מיומנויות פונמיות ולשוניות רבות הכלולות בעיבוד שפה. ה-SLP צריך לחקור את ההבחנה הפונמית הקדם-לשונית, כמו גם מיומנויות לשוניות סמנטיות המתאימות לגיל הפרט. כמה דוגמאות לכלי הערכה פונמית עשויות להיות מבחן המודעות הפונולוגית או המבחן המקיף של עיבוד פונולוגי. מבחני עיבוד שפה יכולים לכלול את ההערכה המקיפה של השפה המדוברת או מבחן עיבוד השפה. המטרה בהערכת SLP צריכה להיות לזהות את רמת הפירוק בתחומים הפונטיים ו/או הלשוניים כדי למקד התערבות ממוקדת.
13. האם תוכל לסכם את הרצף של הפרעות עיבוד כדי להבדיל בין ההיבטים השונים?
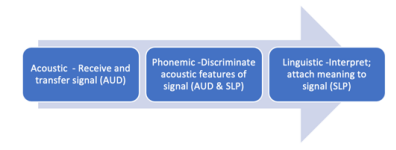
ישנן מיומנויות רבות ושונות הכלולות בעיבוד מידע שמיעתי. זה יכול להיות מכריע עבור איש מקצוע המנסה להבין מהם החסרונות הספציפיים שתורמים לאתגרים שחווה האדם. מבחינה קלינית, קל יותר לקבץ את מרכיבי העיבוד לשלושה סוגים עיקריים - אקוסטיים, פונמיים ולשוניים. ראשית הגירוי האקוסטי חייב להתקבל או להיתפס על ידי האדם. שנית, הוא מועבר מהאוזן הפנימית דרך גזע המוח דרך מערכת העצבים השמיעתית המרכזית אל הקורטקס העליון. אז האונה הטמפורלית הופכת למבנה הקורטיקלי העיקרי המעורב בפענוח ניתוח, ובפירוש האות השמיעתי המתקבל. בעוד שעיבוד המידע השמיעתי אינו התקדמות ליניארית לחלוטין ובהחלט יש חפיפה, זה עוזר למקד את תהליך ההערכה והתערבות אם אתה מקבץ את המרכיבים העיקריים של העיבוד לנתחים אקוסטיים, פונמיים ולשוניים. קיימת גם חפיפה באחריות המקצועית להערכת מיומנויות עיבוד ברצף, מה שמוביל לבלבול מסוים באבחון.
עיבוד אקוסטי מתייחס ליכולת לקבל את האות השמיעתי ולהעבירו שלם לקליפת המוח העליונה. אז האדם יכול לעבוד על הבנת המסר או המשמעות המוטבעים ברצף הצליל הזה. אם האות נפגע או מבולבל במהלך ההעברה הנוירולוגית, אז האדם שומע גובלדיגוק! בגלל זה הם לא יכולים להבין מה נאמר. עיבוד אקוסטי הוא היכולת להבחין בין התכונות השונות של גירוי שמיעתי. תחום זה הוא באחריותו של אודיולוג להעריך.
עיבוד פונמי מתייחס ליכולת להבחין ולתפעל את מקטעי הצליל השונים של השפה, במיוחד העיצורים והתנועות. זה גם חופף לסמלים הגרפיים המייצגים את הצלילים האלה. עיבוד פונמי הוא הבסיס לאוריינות - קריאה, איות ושפה כתובה. זהו תחום קריטי בעיבוד שיש לו השפעה עצומה על הביצועים האקדמיים. ילדים חייבים להיות מסוגלים לשמוע את הצלילים השונים, לייצג אותם באמצעות אות ולרצף אותם ליצירת מילים. בלבול מסוים מתרחש בתוויות אבחנתיות מכיוון שניתן להעריך אזור זה הן על ידי האודיולוג והן על ידי פתולוג שפת הדיבור. אם הפרעת עיבוד פונמית ניכרת לאודיולוג, האבחנה תהיה הפרעת עיבוד שמיעתי. אם הפרעת עיבוד פונמית ברורה לפתולוג שפת הדיבור, היא מאובחנת כהפרעה בעיבוד שפה. מה שהכי חשוב הוא לזהות את החסר הספציפי כפונמי, ולא אקוסטי או לשוני, ולכן ההתערבות מתמקדת בחלק המתאים של רצף העיבוד.
עיבוד לשוני עובר להיבטים הסמנטיים והתחביריים של השימוש בשפה. זה המקום שבו יש לפרש את רצף הצלילים המתקבל כך שיביא לתמונות במוח! הפרט חייב להיות בעל ידע בקוד השפה - או מה המשמעות של רצפי צלילים מסוימים כאשר מילה נאמרת. רכישת השפה מתחילה ב-a
רמה מאוד קונקרטית של שמות עצם ופעלים שניתן לראות ולחוות בקלות. אבל השפה עוברת במהירות למערכות יחסים מופשטות, ואז עיבוד השפה הופך למאתגר יותר. הבנת השפה הופכת מופשטת ומורכבת יותר עם הזמן. הערכת עיבוד השפה היא באחריותו של פתולוג שפת הדיבור. משימות ההערכה ישתנו בהתאם לציפיות השפה מהאדם לפי גיל או התפתחות.
סיכום חזותי של הרצף מסופק להלן (ריצ'רד, 2019).
14. האם יש דרך מהירה לסנן את הרצף כדי שאדע היכן אני צריך להשקיע את זמן האבחון שלי?
כן. מבחן ההקרנה הדיפרנציאלי לעיבוד (DSTP) (Richard & Ferre, 2006) תוכנן בשיתוף עם ד"ר Jeanne Ferre, אודיולוגית, כדי לבצע הערכה מהירה של שלושת ההיבטים העיקריים של רצף העיבוד. הוא כולל 3 מבחנים משנה בעיבוד אקוסטי, שני מבחנים משנה בעיבוד פונמי ושלושה מבחנים משנה בעיבוד לשוני. זֶה
מכשיר ההערכה מיועד לניהול באמצעות CD בתנאי אוזניות תוך כ-35 דקות. זה מאפשר ל-SLP להסתכל במהירות על שלושת תחומי העיבוד העיקריים (אקוסטי, פונמי, לשוני). אם האדם נכשל באחת מתת-מבחנים, ה-SLP יכול לבלות זמן הערכה אבחנתי מעמיק יותר באזור הממוקד שזוהה על ידי כלי המיון.
15. מהם המרכיבים החיוניים לטיפול בהפרעות עיבוד?
חשוב שיהיו תמיד שני סוגים עיקריים של מטרות בעבודה על הפרעות עיבוד. התחום הראשון הוא ליישם אסטרטגיות פיצוי כדי לעזור לאדם להתמודד עם ציפיות יומיומיות. אלה יתואמו עם מורה או הורים כדי לספק סביבה תומכת יותר המגדילה את ההזדמנויות לאדם להבין ולהגיב במדויק למידע שמיעתי. התחום השני הוא לטפל במיומנויות הספציפיות שהן חלשות או בחסר. על מטרות אלו יעבדו ישירות עם הפרט בטיפול. ישנן גם מספר תוכנות מחשב שניתן להשתמש בהן כדי לאפשר לאדם לעבוד באופן עצמאי על מיומנויות עיבוד מחוץ לטיפול, כגון Hear Builder (סופר דופר פרסומים) ו-Hooked on Phonics.
16. מהן כמה מהמיומנויות והאסטרטגיות לעבודה על הפרעת עיבוד שמיעתי? להלן כמה דוגמאות למיומנויות שאתה עשוי לעבוד עליהן עבור הפרעת עיבוד שמיעתי:
זיהוי צליל - צלילים גבוהים לעומת צלילים נמוכים; דפוסי גובה ורצפים. דיבור ברעש – זיהוי מילים המוצגות ברעש ועם מסרים מתחרים.
אבחנה של פונמה – זיהוי עיצורים ותנועות בבידוד והברות.
עיבוד זמני - זיהוי אם יש פונמה אחת או שתיים על סמך קצב ההצגה. לוקליזציה שמיעתית- זיהוי הכיוון ממנו מגיע הצליל.
אסטרטגיות לניהול הפרעת עיבוד השמיעה בסביבה יתמקדו בדרכים למקסם או לשפר את האות. דוגמאות יכללו ישיבה מועדפת, הגברה, חזרות, מתן גיבוי חזותי למידע שמיעתי ושליטה ברעשי רקע.
17. מהן כמה מהמיומנויות והאסטרטגיות לעבודה על בעיית עיבוד פונמי?
הנה כמה דוגמאות למיומנויות שאתה עשוי לעבוד עליהן עבור הפרעת עיבוד פונמי:
ניתוח שמיעתי/פילוח- זיהוי פונמות ספציפיות במיקומי מילים, כגון הצליל הראשון, הצליל האחרון, התנועות האמצעיות או כמה צלילים יש במילה.
סגירה שמיעתית - מילוי צלילים חסרים, כגון "בוטנים - בוטנים ו-elly".
סינתזה/מיזוג שמיעתי - חיבור צלילים מבודדים ליצירת מילים.
זיכרון שמיעתי - יכולת לזכור רצפים של פריטים או מידע ספציפי.
אבחנה שמיעתית – יכולת להבחין בין צלילים במילים, כגון זיהוי הצליל הראשון במילה או אם שתי מילים מסתיימות באותו צליל.
חריזה - מניפולציה של צלילים ראשוניים תוך שמירה על שאר רצף הצלילים של המילה.
אסטרטגיות לניהול בעיות עיבוד פונמיות דומות לאסטרטגיות העיבוד השמיעתי המשפרות או מדגישות את תכונות הצליל. בנוסף, ספק רמזים ויזואליים כגון הגרפמות/אותיות החזותיות כדי להשלים את המידע השמיעתי.
18. מהן כמה מהמיומנויות והאסטרטגיות לעבודה על בעיית עיבוד שפה?
נוכל לפרט אינספור מיומנויות שפה ספציפיות שניתן לטפל בהן. כמה מיומנויות עיקריות האופייניות ברמה היסודית הן הבאות:
מושגים – זיהוי מאפיינים מופשטים של גודל, צורה, מרקם, זמן, כמות, איכות.
סיווג - קיבוץ פריטים לפי תכונות משותפות, כגון פונקציה, צבע, מיקום.
אנטונימים ומילים נרדפות - הבנת יחסי מילים של ההפך או זהה.
השווה וניגוד - זיהוי מאפיינים דומים ושונים בין פריטים.
ריבוי משמעויות - זיהוי משמעויות שונות של מילים על סמך הקשר.
ניבים - משמעויות לא מילוליות של השפה.
ההיבט החשוב בעבודה על מיומנויות הוא לסדר את מטרות השפה בהיררכיה של מורכבות. לדוגמה, תלמיד שיש לו חסרונות בסיווג צריך לשלוט במיומנות הזו לפני שהוא מוכן לעבוד על השוואה וניגוד,
אסטרטגיות לשיפור עיבוד השפה כוללות מתן רמזים או רמזים שיעזרו לתלמיד לאחזר מידע, הוראה בסגנון רב-מודאלי עם חומרים חזותיים והדגמות המתאימות למצגת השמיעתית, הסרת לחץ זמן כדי לעודד זמן חשיבה זהיר, וניסוח מחדש, חזרה, או הרחבה כדי להבהיר הנחיות או מידע.
19. האם לאדם יכול להיות גם בעיה שמיעתית וגם בעיית עיבוד שפה?
כן. אדם יכול לחוות כל שילוב של ליקויים בהפרעת עיבוד. לאדם יכול להיות רק חוסר במיומנויות אקוסטיות, פונמיות או לשוניות. לאדם יכול להיות ליקויים בשני תחומים, כגון עיבוד שמיעתי ופונמי. במקרה זה, האדם היה נאבק באבני הבניין של המידע השמיעתי המחייבים אותו להבחין בתכונות אקוסטיות. זה ישפיע על קריאה, איות ושפה כתובה, אבל הם יכולים להיות מוכשרים במצבים תפקודיים יומיומיים בהבנת שפה מילולית. כאשר לאדם יש גירעונות בכל שלושת התחומים, ההתקדמות בדרך כלל איטית והביצועים האקדמיים מושפעים באופן משמעותי (ריצ'רד, 2017).
20. האם הטיפול יעיל לטיפול בהפרעות עיבוד?
המחקר על יעילות הטיפול בהפרעות עיבוד מעורב מאוד. מכיוון שההפרעה כה רחבה וכוללת היבטים רבים ושונים של כישורי שמיעה ושפה, קשה להראות השפעות טיפול חזקות. אין הסכמה טובה כיצד להגדיר את ההפרעות בתוך הדיסציפלינות של אודיולוגיה ופתולוגיה של שפת הדיבור. כתוצאה מכך, קבוצת האנשים שאובחנו עם הפרעת עיבוד ועשויה להיכלל במחקר מחקר נוטה להיות הטרוגנית מאוד, ומצמצמת את ההזדמנות להפגין יעילות טיפול חזקה. כאשר מוצעת הפרעת עיבוד, חשוב להעריך קלינית את מיומנויות החסר הספציפיות שתורמות לאבחנה זו. הטרמינולוגיה של "הפרעת עיבוד שמיעתית (APD)" או "הפרעת עיבוד שפה (LPD)" יכולה להיות מטעה, תלוי מי הציג את התווית. בשני המקרים, APD או LPD, מיומנויות מרובות מוקפות תחת התווית הזו. התערבות תהיה יעילה רק אם הטיפול ממוקד בתחום העיקרי של הליקוי (פונמי אקוסטי, לשוני) ומכוון למיומנויות תפקודיות.
Course Description
There is a good deal of confusion among audiologists and speech-language pathologists when a diagnosis of “processing disorder” is introduced. This course presents a continuum model to differentiate processing disorders into acoustic, phonemic, or linguistic aspects so that assessment and treatment can become more focused and effective. The roles of audiologists and SLPs in relation to processing disorders are described, and compensatory strategies for differing aspects of processing are presented.
Presenters
Gail J. Richard, PhD, CCC-SLP
From the Desk of Ann Kummer

I am so excited about this 20Q article because there

continues to be a lot of confusion among both
audiologists and speech-language pathologists
regarding the diagnosis of a “processing disorder.” We
use terms such as “auditory processing disorder,”
“central auditory processing disorder,” “language
processing disorder” and “phonemic processing disorder,” but we are not always clear on
how these disorders and terms are differentiated. Fortunately, Dr. Gail J. Richard, Ph.D.,
CCC-SLP will answer our questions about processing disorders with this 20Q article.
Here’s a little information about Dr. Richard. She is emeritus professor at Eastern Illinois University in Charleston, IL, where she was on the faculty for 37 years specializing in childhood developmental language disorders, such as autistic spectrum disorders, auditory/language processing, executive functions, and selective mutism. She also founded the Autism Center at the university and a program for college students with autism spectrum disorder – Students with Autism Transitional Education Program (STEP). She has numerous publications and is a frequent conference presenter, sharing her practical clinical perspective. Professional awards include Honors of the American Speech-Language-Hearing Association, recipient of the Illinois Clinical Achievement Award, and multiple teaching awards. She has also held many leadership positions in professional organizations, including President of the American Speech-Language-Hearing Association in 2017.
In this article, Dr. Richard will use a continuum to explain processing disorders that involve acoustic, phonemic, and/or linguistic aspects. She discusses the responsibilities of an audiologist and speech-language pathologist in relation to processing disorders. Most importantly, she gives examples of specific skills and compensatory strategies that can be used for the different types of processing disorders.
This course will definitely help you to differentiate processing disorders based on acoustic, phonemic, or linguistic aspects. As a result, your assessment and treatment will become more focused and effective.
Now…read on, learn, and enjoy!
https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 1/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com
Ann W. Kummer, PhD, CCCSLP, FASHA, 2017 ASHA Honors
Contributing Editor
Browse the complete collection of 20Q with Ann Kummer CEU articles at www.speechpathology.com/20Q
20Q A Continuum Approach for Sorting Out Processing Disorders
Learning Outcomes
After this course, readers will be able to:
Define and differentiate auditory and language processing disorders
Utilize a continuum to describe different aspects of processing into acoustic, phonemic, and linguistic Identify the responsibilities of an audiologist and speech-language pathologist in relation to processing disorders List examples of specific skills and compensatory strategies within the acoustic, phonemic, and linguistic aspects of processing
1. What is a “processing disorder?”

A “processing disorder” is actually a generic term that is used by many professionals to describe a variety of learning problems. Psychologists, teachers, audiologists, and speech-language pathologists all introduce the term when an individual is having difficulty accurately
understanding and responding to sensory information. Unfortunately, there are a number of different skills that are encompassed within the term “processing disorder “which leads to a lot of
Gail Richard
confusion.
2. Are there different types of processing disorders?
Absolutely! We process information from all our sensory systems. We can close our eyes and taste, smell or feel something to try and figure out what it is. In aphasia literature, we talk about agnosia – when you receive a stimulus but can’t comprehend or make sense of it. It is easier to comprehend in the visual (sight), tactile (touch), olfactory (smell), and gustatory (taste) senses because they remain there while you work on attaching meaning to the stimulus. Auditory information is harder to process because it is so transient – it is gone very quickly. Then we add the aspect of auditory information being in a language code. Other than environmental noises, auditory stimuli require more cognitive energy to understand. Most of the challenges that negatively affect learning and functioning in the everyday world are in the area of auditory processing.
3. What is auditory processing?
When “auditory processing” was first introduced (Mylebust, 1954) it was used to describe children who had normal hearing but were struggling to understand auditory information presented to them. They could hear the words but had trouble attaching meaning to understand the message within the language. The term was very broad in its definition. It referred to interference with comprehension of language that could be based in language, academic learning, or listening skills. For decades the term “auditory processing” was defined as problems abstracting meaning from an auditory stimulus (Massaro, 1975), which encompassed many cognitive and language abilities.
As the discipline of audiology developed, professionals wanted to better differentiate the auditory and language components. The first step was to emphasize that the individual must have normal hearing acuity in the peripheral auditory system. In other words, the person can accurately receive an auditory stimulus but struggles to understand or interpret the signal. “Central auditory processing” was introduced (Keith, 1977) to specify that the deficits were based in auditory skills mediated in the central auditory nervous system (CANS). The difficulty in discriminating various features of the acoustic signal were subsequently interfering with comprehension of the message.
4. What do you mean by acoustic features of the signal?
https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 2/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com
When we analyze an acoustic stimulus, there are many aspects that contribute to the integrity of the sound. Pitch, loudness, speed of presentation, and the different phonemes all occur together very quickly. An individual needs to be able to discriminate the different sound segments to accurately attach meaning. For example, I need to be able to hear the difference in “p” versus “b” to know if the word I heard was “pat” or “bat”. My interpretation of the message will be confused if I can’t tell those sounds apart. The picture in my brain will be formed by how I hear and interpret a sound sequence. The sound sequence will have meaning based on the language code.
5. Can you give me some examples of the acoustic skills that are part of an auditory processing disorder?
An audiologist would look for poor performance in the ability to localize sound, the ability to discriminate different phonemes, trouble hearing when the signal is compromised by static or background noise, or trouble hearing when there is more than one signal at a time.
6. Are the acoustic features part of the definition for central auditory processing disorder?
Yes, audiologists and speech-language pathologists gradually acknowledged that there were acoustic, phonemic, and linguistic aspects to processing. Audiology focused on the acoustic and phonemic aspects of auditory processing. Neurologically their definition focused on moving the acoustic signal from the inner ear through the central auditory nervous system to the upper cortex. The definition for auditory processing is “the perceptual processing of auditory information in the central nervous system (CNS) and the neurobiological activity that underlies that processing and gives rise to electrophysiologic auditory potentials (ASHA, 2005a). Basically, auditory processing is the efficiency and effectiveness in how the central auditory nervous system utilizes auditory information.
7. Are “auditory processing” and “central auditory processing” the same thing?
Yes, there is agreement in audiology that those are synonymous terms. For a while central was included in parentheses, so you would see (central) auditory processing or (C)AP. This was to emphasize the focus on central auditory nervous system (CANS) skills when referring to an auditory processing disorder. The recommendation (ASHA, 2005b) was to drop central and just use auditory processing (AP) and auditory processing disorder (APD) without the use of central.
8. Who can diagnose an auditory processing disorder?
An audiologist is the only professional who can diagnose an auditory processing disorder. While numerous professionals might suggest that an individual has an auditory processing disorder, they are describing the types of activities that are problematic for a person. A teacher, psychologist or physician might observe that an individual is having trouble understanding what is said to them and state that they have an auditory processing disorder, but that is not a diagnosis. It is a professional opinion of what could be the problem. Referral for a formal evaluation should be considered.
9. What does the evaluation for assessing an auditory processing disorder involve?
The purpose of an auditory processing evaluation is to assess the integrity of the central auditory nervous system in a controlled discrete manner. The tests stress the auditory system by compromising the acoustic signal to see how the individual responds. Each audiologist designs a battery of tests that he or she believes will adequately assess the individual’s auditory processing ability. There are four types of procedures that can be used in a central auditory processing evaluation:
Monotic/monaural – acoustic stimuli presented to one ear;
Dichotic – different acoustic stimuli presented simultaneously to both ears, such as “hot” in the left ear and “dog” in the right ear at the same time;
Binaural interaction – separate signals to each ear must be added together or separated, such as “m” to the left ear, “a” to the right ear, and “t” to the left to the word “mat”;
Electrophysiological – these are neurological reflex tests that do not require a response from the individual; electrodes are attached to evaluate brain stem responses.
There is not a consensus battery within audiology regarding which skills should be included in an evaluation. However, the rule of thumb for diagnosis of an auditory processing disorder is a performance deficit of 2 standard deviations below the mean on two or more tests of the battery administered to the person.
10. What is the role of the speech-language pathologist in auditory processing disorders APD?
https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 3/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com
While an audiologist is responsible for diagnosing an auditory processing disorder, it is usually a speech-language pathologist (SLP) who is responsible for coordinating and providing treatment to address the auditory processing deficits. That is why it is important to know which auditory skills were significantly impaired that resulted in the diagnosis of APD. There are many aspects to an auditory processing evaluation that examine the person’s ability to discriminate various acoustic features. The SLP needs to work with the audiologist to identify the most pertinent aspects that will functionally make a difference.
11. What is the difference between language processing and auditory processing?
Processing an acoustic signal is very different than processing a linguistic signal. Auditory processing typically requires little to minimal interpretation of the auditory stimulus. Sometimes a simple repetition task will tell you that the signal was transferred accurately through the brainstem to the upper cortex. The central nervous system has incredible neurological redundancy that minimizes the possibility of deficits in transferring the signal to the temporal lobe. Most auditory processing disorders occur once the individual begins to discriminate and manipulate the acoustic features in the upper cortex at a phonemic level. The acoustic signal is usually not the source of the problem. The difficulty is when the individual tries to decode and interpret the message within the auditory signal. That is language processing. Language processing is the ability to attach meaning to the acoustic stimulus. It is the ability to understand the semantic and syntactic message encoded in the signal. Many of the learning difficulties experienced by children in an academic setting are based in difficulty processing language.
12. Who diagnoses language processing disorders?
The speech-language pathologist is responsible for conducting an evaluation to see if the deficits are in phonemic or linguistic aspects of processing. The speech-language pathologist will conduct assessment procedures to evaluate phonemic discrimination and manipulation of sounds as well as language comprehension. There is not one assessment instrument that will provide the necessary information, so the SLP must also rely on a battery of tests, like what the audiologists does in assessment. There are numerous phonemic and linguistic skills that are encompassed within language processing. The SLP should probe pre-linguistic phonemic discrimination as well as semantic linguistic skills that are age-appropriate for the individual. Some examples of phonemic assessment tools might be the Phonological Awareness Test or Comprehensive Test of Phonological Processing. Language processing tests could include the Comprehensive Assessment of Spoken Language or Language Processing Test. The goal in the SLP assessment should be to identify the level of breakdown in the phonetic and/or linguistic areas to focus targeted intervention.
13. Can you summarize the continuum of processing disorders to differentiate the various aspects?
There are many different skills that are encompassed within processing auditory information. It can be overwhelming to a professional trying to figure what the specific deficits are that contribute to the challenges being experienced by the person. Clinically, it is easier to group the components of processing into three main types – acoustic, phonemic, and linguistic. First the acoustic stimulus must be received or perceived by the person. Second, it is transferred from the inner ear through the brain stem via the central auditory nervous system to the upper cortex. Then the temporal lobe becomes the primary cortical structure involved in decoding analyzing, and interpreting the auditory signal received. While the processing of auditory information is not completely a linear progression and there is certainly overlap, it helps to focus the assessment and intervention process if you group the major components of processing into acoustic, phonemic, and linguistic chunks. There is also overlap in professional responsibilities for evaluating processing skills in the continuum, which leads to some confusion in the diagnosis.
Acoustic processing refers to the ability to receive the auditory signal and transfer it intact to the upper cortex. Then the person can work on understanding the message or meaning embedded in that sound sequence. If the signal become compromised or messed up during the neurological transference, then the person hears gobbledygook! That’s why they can’t understand what was said. Acoustic processing is the ability to discriminate the various features of an auditory stimulus. This area is the responsibility of an audiologist to evaluate.
Phonemic processing refers to the ability to discriminate and manipulate the different sound segments of the language, specifically the consonants and vowels. It also overlaps into the grapheme symbols that represent those sounds. Phonemic processing is the foundation for literacy – reading, spelling, and written language. This is a critical area of processing that has a huge impact on academic performance. Children must be able to hear the different sounds, represent them with a letter, and sequence them to form words. Some confusion occurs in diagnostic labels since this area can be evaluated by both the audiologist and speech-language pathologist. If a phonemic processing disorder is evident to the audiologist, the diagnosis will be auditory processing disorder. If a phonemic processing disorder is evident to the speech-language pathologist, it is diagnosed as a language processing disorder. What is
https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 4/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com
most important is to identify the specific deficit as being phonemic, rather than acoustic or linguistic so intervention is focused on the appropriate part of the processing continuum.
Linguistic processing transitions into the semantic and syntactic aspects of language use. This is where the sound sequence received must be interpreted to result in pictures in the brain! The individual must have knowledge of the language code – or what certain sound sequences mean when a word is spoken. Language acquisition begins at a
very concrete level of nouns and verbs that are easily seen and experienced. But language quickly transitions into abstract relationships and that’s when language processing becomes more challenging. Comprehension of language becomes more abstract and complex over time. Evaluation of language processing is the responsibility of the speech-language pathologist. The assessment tasks will vary based on the language expectations for the individual by age or development.
A visual summary of the continuum is provided below (Richard, 2019).
14. Is there any quick way to screen the continuum so I know where I need to spend my diagnostic time?
Yes. The Differential Screening Test for Processing (DSTP) (Richard & Ferre, 2006) was designed in collaboration with Dr. Jeanne Ferre, audiologist, to do a quick evaluation of the three major aspects of the processing continuum. It includes 3 subtests in acoustic processing, two subtests in phonemic processing, and three subtests in linguistic processing. This
assessment instrument is designed to be administered by CD under headphone conditions in about 35 minutes. This allows the SLP to quickly look at the three main areas of processing (acoustic, phonemic, linguistic). If the individual fails any of the subtests, the SLP can spend more in-depth diagnostic assessment time in the focused area identified by the screening tool.
15. What are the essential components for treating processing disorders?
It is important to always have two main types of goals when working on processing disorders. The first area is to implement compensatory strategies to help the person cope with everyday expectations. These would be coordinated with a teacher or parents to provide a more supportive environment that increases the opportunities for the person to accurately understand and respond to auditory information. The second area is to address the specific skills that are weak or in deficit. These goals would be worked on directly with the individual in therapy. There are also several computer programs that can also be utilized to let the person work independently on processing skills outside of therapy, such as Hear Builder (Super Duper Publications) and Hooked on Phonics.
16. What are some of the skills and strategies to work on an auditory processing disorder? Here are some examples of skills you might work on for an auditory processing disorder:
Pitch identification– high pitched tones versus low pitched tones; pitch patterns and sequences. Speech in noise – identifying words presenting in noise and with competing messages.
Phoneme discrimination – identifying consonants and vowels in isolation and syllables.
Temporal processing– identifying if there is one phoneme or two based on rate of presentation. Auditory localization- identifying the direction of where sound is coming from.
Strategies to manage the auditory processing disorder in the environment would focus on ways to maximize or enhance the signal. Examples would include preferential seating, amplification, repetition, providing visual back-up to auditory information, and controlling background noise.
17. What are some of the skills and strategies to work on a phonemic processing problem?
https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 5/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com Here are some examples of skills you might work on for a phonemic processing disorder:
Auditory analysis/segmentation- Identifying specific phonemes in word positions, such as the first sound, last sound, middle vowel, or how many sounds are in a word.
Auditory closure – filling in missing sounds, such as “peanut -utter and -elly”.
Auditory synthesis/blending – putting isolated sounds together to form words.
Auditory memory – ability to remember sequences of items or specific information.
Auditory discrimination – ability to distinguish between sounds in words, such as identifying the first sound in a word or if two words end with the same sound.
Rhyming – manipulating initial sounds while maintaining the rest of the word’s sound sequence.
Strategies to manage phonemic processing problems are similar to the auditory processing strategies that enhance or emphasize the sound features. In addition, provide visual cues such as the visual graphemes/letters to supplement the auditory information.
18. What are some of the skills and strategies to work on a language processing problem?
We could list innumerable specific language skills that could be addressed. A few major skills that are typical at the elementary level are the following:
Concepts – identifying abstract features of size, shape, texture, time, quantity, quality.
Categorization - grouping items by shared attributes, such as function, color, location.
Antonyms & Synonyms – understanding word relationships of the opposite or same.
Compare & contrast – identifying similar and different features between items.
Multiple Meanings – recognizing different meanings of words based on context.
Idioms – nonliteral meanings of language.
The important aspect in working on skills is to order the language goals in a hierarchy of complexity. For example, a student who has deficits in categorization needs to master that skill before they are ready to work on comparing and contrasting,
Strategies to enhance language processing include providing clues or hints to help a student retrieve information, teaching in a multi-modality style with visual materials and demonstrations to go with the auditory presentation, removing time pressure to encourage careful thinking time, and rephrasing, repeating, or expanding to clarify directions or information.
19. Can an individual have both an auditory and language processing problem?
Yes. An individual can experience any combination of deficits in a processing disorder. The person could have only a deficit in acoustic, phonemic, or linguistic skills. An individual could have deficits in two areas, such as auditory and phonemic processing. In this case, the person would be struggling with the building blocks of the auditory information that require them to discriminate acoustic features. This would impact reading, spelling, and written language, but they could be competent in everyday functional situations in understanding verbal language. When an individual has deficits in all three areas, progress is generally slow and academic performance is significantly impacted (Richard, 2017).

https://www.speechpathology.com/E/10008/1082891/190ab775068b3f947b 6/7
3/21/22, 3:06 PM 20Q: A Continuum Approach for Sorting Out Processing Disorders - SpeechPathology.com
20. Is treatment effective for addressing processing disorders?
The research on treatment efficacy for processing disorders is very mixed. Because the disorder is so broad and includes many different aspects of auditory and language skills, it is difficult to show strong treatment effects. There is not good agreement in how to define the disorders within the disciplines of audiology and speech-language pathology. Consequently, the group of individuals diagnosed with a processing disorder who might be included in a research study tend to be very heterogeneous, minimizing the opportunity to demonstrate strong treatment efficacy. When a processing disorder is suggested, it is important to clinically evaluate the specific deficit skills that contribute to that diagnosis. The terminology of “auditory processing disorder (APD)” or “language processing disorder (LPD)” can be misleading, depending on who introduced the label. In both cases, APD or LPD, multiple skills are encompassed under that label. Intervention will only be effective if the treatment is focused in the major area of deficit (acoustic phonemic, linguistic) and targets functional skills.

Comments
Post a Comment